Envelope (Sulcular) Flap — Design Principles and Clinical Considerations
Overview
The envelope flap, also known as a sulcular flap, is one of the most frequently employed flap designs in oral surgery and periodontics. It allows access to the alveolar bone and root surfaces while maintaining optimal vascular integrity and minimal postoperative morbidity.
Key Design Considerations
1. Incision Extension
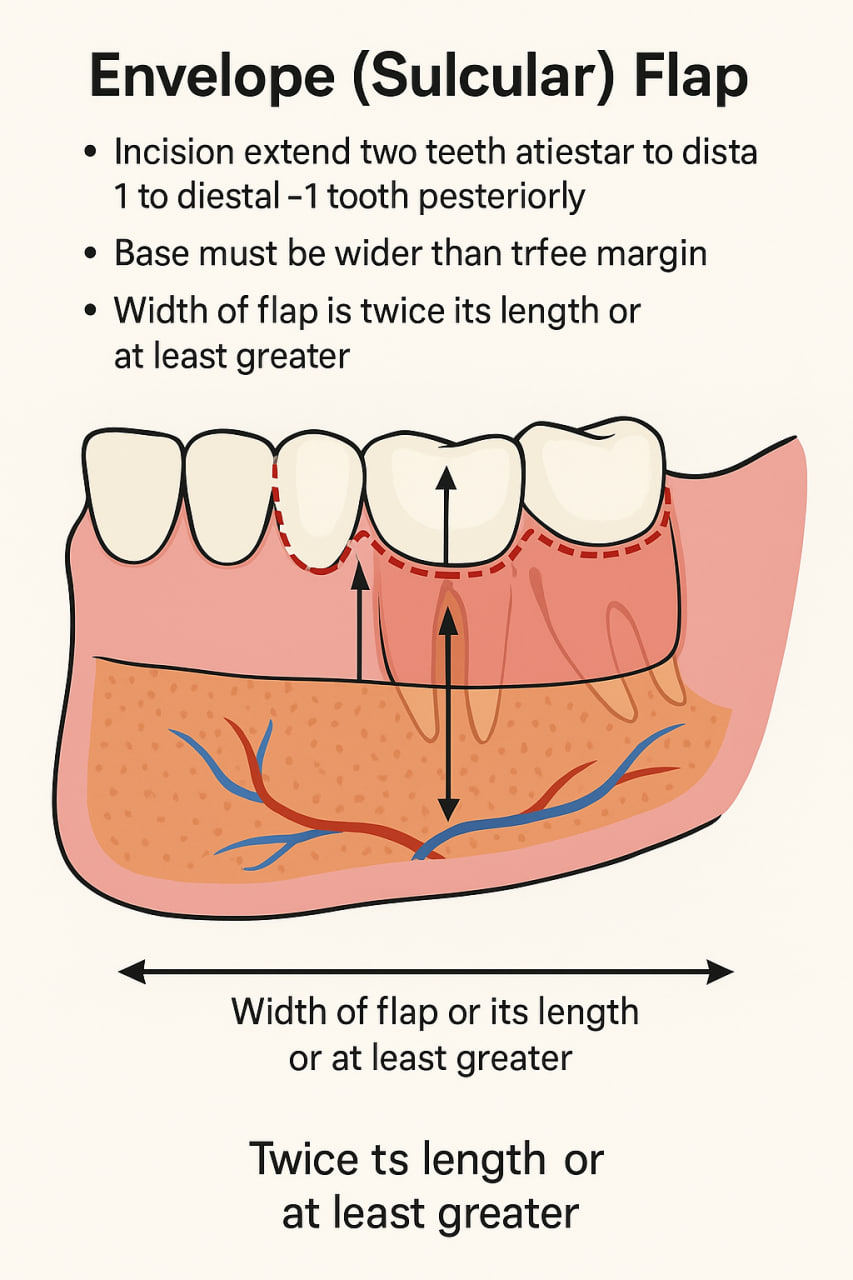
The incision should extend two teeth anteriorly and one tooth posteriorly to the target tooth.
This length ensures adequate visibility and access for instrumentation while minimizing excessive tissue tension during reflection.
2. Flap Base and Blood Supply
The base of the flap must always be wider than its free (coronal) margin.
This design maintains a broad vascular connection from the underlying periosteum, preventing ischemia or necrosis of the marginal tissues. A narrow-based flap risks compromising perfusion, particularly at the crestal edge.
3. Flap Proportions
The width of the flap (mesiodistal dimension) should ideally be twice its length (apicocoronal dimension), or at least greater than the vertical extent.
This proportion enhances flap stability and ensures sufficient tissue flexibility for retraction and repositioning without tearing.
 Flap 1")
Clinical Notes
-
Always employ a sharp #15C or microsurgical blade to preserve the scalloped gingival margin.
-
Maintain submarginal incisions parallel to the long axis of the tooth to protect papillary integrity.
-
The flap reflection should be gentle, using a periosteal elevator to preserve the periosteum where feasible.
References: